ABSTRACT
-
Background
After encountering funding problems in the 1980s, the French healthcare system is now facing new types of public problems that trigger organizational responses. This is the case with the growing shortage of medical workforce since the 2000s—particularly GPs—leading to geographical inequalities in access to primary care. The expression “medical desert” has since flourished in political discourse and the press, contributing to the dramatization of the problem and pushing it to the top of the political agenda. At the same time, we are witnessing the development of a new repertoire of policy instruments that make primary care—and GPs in particular—the cornerstone of the healthcare system.
-
Objective
Based on an empirical qualitative analysis, this paper highlights the key role played by a new “instrument constituency” (
Béland & Howlett, 2015;
Voß & Simons, 2014) in the primary care reform process. This constituency consists of a small group of GPs —open to team-based practice, the integration of psychosocial dimensions of health, and changes in payment methods— playing the role of professional entrepreneurs, and the established “Welfare elite” —composed of political actors and civil servants who share reform objectives regarding health policies.
-
Approach
The paper adopts a processual approach, first focusing on the formation of this instrument constituency (around a specific organizational model: the multi-professional healthcare centers), then its gradual institutionalization through successive reforms (e.g., new financing methods and territorial integration of healthcare services) and the evolution of this instrument constituency (more specifically, the evolution of the roles and positions of its members).
-
Findings
The instrument constituency progressively institutionalized through new financing methods and territorial integration of healthcare services, extending to new professional and political actors. However, the persistence of the “medical deserts” problem and the proliferation of competing policy instruments have recently weakened this constituency.
-
Implications
The paper raises the question of the constituency’s sustainability in the current context of increasing conflicts in the French healthcare system, and opens a broader discussion on the role of instrument constituencies in policy change.
-
Keywords: instrument constituency; policy change; primary care reform; professional entrepreneurs; medical deserts; multiprofessional healthcare centers (MSPs); Bismarckian healthcare system; welfare elite; France
Introduction
In the French Bismarckian healthcare system, state intervention has long been limited to the regulation of the hospital sector, without extending to the organization and financing of the outpatient sector and more specifically primary care. However, the system has witnessed major changes since the 1980s, through the strengthening of the State’s role over social partners—managing the sickness funds—and healthcare providers in ambulatory care. In this long-term transformation process, a group of senior civil servants—characterized as a programmatic “Welfare elite” (
Genieys & Hassenteufel, 2015)—played a key role in the design, adoption, and implementation of a policy change program, that they drafted through several expert commissions, especially the Soubie Commission in the early 1990s. One of the main dimensions of this program was the shaping of new state-led institutions, especially the National Union of Sickness Funds (UNCAM
1) and the Regional Health Agencies (ARS
2), as well as new policy instruments, such as the annual Social Security Financing Laws (LFSS
3). Back then, the main issue tackled by these institutional changes was the control of health insurance expenditure. However, this dominant orientation in the policy agenda has been progressively challenged at the turn of the 2000s, with the emergence of new public problems related to inadequate care coordination and shortcomings in primary care provision, especially regarding general practitioners (GPs). “Medical deserts”—a dramatic expression (
Hassenteufel et al., 2020a) referring to the difficulty of access to GPs in certain geographical areas, most commonly rural areas and disadvantaged urban neighborhoods—began to spread in the press and in political discourse, and remains at the forefront of media attention to this day (
Moyal, 2024).
Successive governments have promoted different solutions to address this problem. In a sector where physicians are mainly self-employed, all these measures are incentive- based: recognizing general practice as a medical specialty, providing financial support for GPs to set up practices in underserved areas, and supporting new forms of professional practice. Among these are multiprofessional health care centers—called “
Maisons de Santé Pluriprofessionnelles”, MSPs. These organizations bring together GPs and allied healthcare providers, most frequently nurses, physiotherapists, chiropodists and midwives. MSPs are inspired by professional initiatives launched locally by GPs who did not wait for the government to intervene before getting organized (
Moyal, 2024). Unlike previous health insurance reforms, in which political and administrative actors played a key role, physicians are driving this change and are supported by the state and the national health insurance fund (CNAM). Legally recognized by the 2007 LFSS, MSPs were more than 2,800 nationwide in 2025, already joined by 17% of French GPs in 2023 (
Bergeat & Cassou, 2023). They are particularly popular among young healthcare providers. These organizations are also the setting for new innovative practices regarding care coordination, health service integration, and participative and community health (
Fournier et al., 2018;
Morize, 2024;
Pitti, 2021).
How can we explain this unprecedented alliance of medical and programmatic actors in the primary care reform process, and more specifically around MSPs? What does this alliance reveal about policy change in this field? How is this alliance evolving over time and what are the implications for medical and programmatic actors as well as the primary care reform process at stake? By answering these questions, this article simultaneously offers an analysis of the reform process of primary care in France and contributes more generally to an agency-based perspective on policy change.
This paper draws on qualitative data collected as part of two different research projects in which the authors participated individually. The data were subsequently cross- referenced and analyzed jointly. They were also updated through interviews with actors previously surveyed in these studies, thereby providing a longitudinal perspective that we consider essential for understanding the evolution of the alliance between the public authorities and the medical profession in this reform process. The first project conducted between 2015 and 2018 (REGMEDPROV
4) aimed to understand the role of physicians’ organizations in the policy response to the medical provision shortage in France and Germany. It enabled the collection of empirical data on the French case: 20 in-depth interviews with administrative experts (working in the health Ministry and sickness fund organizations), political experts (ministerial staffers, specialized parliamentarians in health policy, representatives of local authorities associations), academic experts, and representatives of the main medical associations, a systematic analysis of the public reports (administrative reports, parliamentary reports, reports from associations, reports from research institutions) tackling the issue of medical shortages published from 2000 to 2018 and other public documents produced by the main medical associations, and a press analysis over the same period. The results of this project were combined with a sociological survey conducted from 2016 to 2019
5 focusing more specifically on the emergence and implementation of MSPs in France. This second analysis was conducted on two levels: at the national level, semi-structured interviews with representatives of the programmatic elite and professional organizations (N=29) made it possible to trace the coupling process between MSPs and the “medical deserts” problem, as well as the alignment of medical and public actors around this new organizational model. Among professional representatives, some were clearly in favor of the “MSP solution,” while others were more critical. At the local level, we interviewed GPs leading six different MSP projects (N=10) —some initiating this change alone, while others are partnering with colleagues to carry out these projects). These GPs were, by definition, supportive of this new mode of practicing family medicine and this constitutes an intentional selection bias in this part of the study, which aimed to understand how and why GPs were getting involved in the development of MSPs at the local level. This empirical material (see
appendix) provides a multilevel analysis aimed at understanding the intricate roles of a professional group and the programmatic elite in both the conception and the implementation of primary care reforms and their evolving relationship.
In the first part of the paper, we present the theoretical issues of our agency-based analysis of policy change based on two key concepts: professional entrepreneurs and instrument constituencies. In the second part, we place our analysis in historic context by tracing the preconditions that have led, since the 1990s, to a gradual alignment of a segment of the medical profession with the programmatic elite. In the third part, we focus on the structuration of this instrument constituency around a rather consensual instrument to tackle medical shortages —MSPs —that is legally recognized in 2007. In the fourth part, we consider the gradual institutionalization of this instrument constituency from the middle of the 2000s to the beginning of the 2020s through successive reforms (e.g. new financing methods and new policy instruments fostering territorial integration of health care services). This process is accompanied by the emergence of new instruments and actors involved in primary care policies, as well as an evolution in the roles and positions of its initial members. In the fifth section, we raise the question of the sustainability of this constituency, in the current context of increasing conflicts in the French healthcare system. In the conclusion we open the discussion on the specificities of the French case and the broader implications of the instrument constituency approach for comparative healthcare policy analysis.
The Role of Professional Entrepreneurs and Instrument Constituencies in Policy Change
The theoretical aim of this paper is twofold. First, we tackle the issue of the role of physicians in policy change. The literature on physicians as an interest group tends to emphasize their role as veto players (Tsebelis, 2002), defending their dominant position in the healthcare state (
Moran, 1999) and their professional power (
Freidson, 1970), rather than their role as drivers of policy change. In this empirical research, however, we identified a group of GPs acting as professional entrepreneurs promoting changes in the organization of primary care, in alliance with administrative and political actors. They are not only “policy entrepreneurs” in the sense of Kingdon (
Kingdon, 1984), acting as agenda setters for the issues of access and coordination of primary care and coupling policy instruments to previously identified problems: they are also involved in policy decision and implementation
6. By selecting, translating, recombining, and, most importantly, by promoting policy solutions, they fulfil a genuinely creative and constructive role. Thus, we define these professional entrepreneurs as individual or collective actors coming from a professional group—in this case the medical profession—and actively promoting policy solutions in order to address specific policy problems (
Hassenteufel et al., 2020b), but also leading initiatives locally to make medical practice evolve (
Moyal, 2022). These professional entrepreneurs are embedded in close interactions with the programmatic actors holding key positions in policy design and decision processes, in order to promote specific operational solutions and to influence the policy process by outmaneuvering established organizations representing physicians. We demonstrate that these interactions have led to the structuration of an “instrument constituency” (
Béland & Howlett, 2015;
Voß & Simons, 2014), around a shared policy instrument defined as a key solution to the problem of local shortages in medical provision: the MSPs. Unlike “advocacy coalitions” (
Sabatier and Jenkins-Smith 1993)
7 and policy communities, instrument constituencies are focused on policy solutions, not policy beliefs or problem framing (
Simons & Voß, 2017). According to this approach, actors with different policy goals and ideas can agree on the same policy instrument, especially when it can be interpreted differently because of its ambiguities. The main specificity of the MSP case, which distinguishes it from the market- based policy instruments examined by Simon and Voß (in their case emission trading and network access regulation) is the types of actors involved in this constituency, namely professional, administrative and political actors at the national level, unlike the transnational experts pinpointed in Simon and Voß’ case.
The second theoretical aim of the paper is to examine more broadly the process of change to which this instrument constituency contributes. We show that while these new team-based organizations were not initially designed by GPs to address the problem of medical shortage, this political agenda represented a policy window for this solution to be recognized and supported by public authorities. Our observations thus illustrate Kingdon’s theory of solutions chasing problems (
Béland & Howlett, 2015;
Kingdon, 1984). We also argue that the change enabled by this new instrument—and other instruments that have followed this initial change—is limited but progressive. Far from a paradigmatic change (
Hall, 1993;
Jobert, 1992) in response to what is often presented as a “crisis” of medical shortage, the organization of primary care through this new repertoire of instruments is more a case of incremental change based on a layering process (
Streeck & Thelen, 2005). This results in a complex interplay between a new way of practicing family medicine (in multiprofessional teams, responding to new socio-economic and geographic issues in access to healthcare), corresponding to a new layer in primary care, and the historical model of private medical practice (
Moyal, 2024;
M2026), which has not disappeared but has been progressively transformed and eroded. Another particularity of our case is that the problem of medical deserts has been perpetually on the political agenda since it was first identified in the early 2000s. It has thus been gradually captured by multiple actors (
Gusfield, 1981) promoting different solutions, some of which competing with MSPs and ultimately weakening the instrument constituency that initially emerged around this solution. Therefore, this paper is also a contribution to the study of different instrument constituency dynamics: it examines not only the institutionalization of instrument constituencies—through the creation of institutions and organizations within which their members coordinate their positions and build concrete policy arrangements (
Simons & Voß, 2017) but also their weakening.
From Historical Conflicts with the Medical Profession to Partnership with GPs
The long-standing relation between the government and the medical profession in France has been marked by conflicts over the integration of physicians into the social insurance system, which was established in the late 1920s (
Hassenteufel, 1996;
1997). The Confederation of French Medical Unions (CSMF
8) was created in 1928 to bring together all the unions under the banner of “free medicine” (“
médecine libérale”), expressing their opposition to a Bismarckian health insurance system and promoting freedom for physicians to choose their patients, freedom of prescription, fee-for-service payment, and direct payment by patients. In the 1930 health insurance act, these principles as well as the physicians’ freedom to fix the amount of medical fees were guaranteed, and after the Second World War the principle of freedom of settlement was added.
Despite the creation of the Social Security System in 1945, the French medical profession was successful in maintaining these principles inside the new health insurance system. However, a ministerial decree in 1960 imposed binding-fee schedules negotiated between physicians’ unions and local sickness funds. Since 1971, sickness funds organizations negotiate a national medical agreement (called “
convention nationale”) with the medical unions. One of the main components of this agreement consists of the setting of the physicians’ fees for all procedures and consultations. This negotiation gives established physicians’ organizations a strong institutional power to defend the principles of the “
médecine libérale ” (preserved up to now,
Borgetto, 2011) and, more generally, their economic interests within the French health insurance system.
Like in other policy domains characterized by changes in the morphology of professional groups and controversial policy issues, lines of fragmentation inside the medical profession have grown since the 1970s (
Hassenteufel, 2019). New organizations representing specific parts of the medical profession have been created, such as MG France, representing the interests of GPs, and specific organizations representing young physicians (the
Syndicat National des jeunes médecins généralistes—SNJMG—created in 1991, the
Regroupement Autonome des Généralistes et Jeunes Installés et Remplaçants—ReAGJIR—in 2008, and
Jeunes médecins created in 2016 in order to represent all kind of young physicians).
The creation of a specific GP trade-union, MG France, in 1986 (
Hassenteufel, 2010), can be considered as a precondition for the shaping of an instrument constituency. Opposing the declining role of GPs as a consequence of medical specialization, this union emphasized the need to give GPs a central position in the healthcare system. This is presented both as a way to limit healthcare expenditure and to improve the monitoring of patients as well as the coordination of treatments. The main ideas were to assign to the GP the role of gatekeeper and coordinating physician who should be seen before any specialist consultation, to have a medical file shared among providers, and to institute healthcare networks. These professional proposals were endorsed by political actors. Claude Evin, socialist Minister of Health in the early 1990s, supported the idea of “health contracts” with GPs and tried to include them in the national medical agreement. This failed, however, because of the opposition of the more established physicians’ organizations, representing mostly medical specialists. In 1996, the Prime Minister Alain Juppé then introduced the notion of “referring physician”, based on MG France’s proposal, and allowed the negotiation of a specific collective agreement for GPs in the 1996 Social Security reform. Another important issue for MG France was the strengthening of family medicine in medical education. Family medicine departments were created in medical schools in 1997, but the process of establishing a specific academic curriculum was slow despite the mobilization of the National College of General Practice lecturers (CNGE
9). Family medicine was finally recognized as a new medical specialization in 2004 (
Bloy, 2010). The 2009 HPST Act (Loi “
Hôpital, Patients, Santé et Territoires”)—defining primary care for the first time in France—finally recognized specific responsibilities for GPs, as coordinator of patients’ pathways. It also stated the objective to make all medical students do an internship in general practice. These developments were the result of close contacts between MG France leaders and the then right-wing Health Minister Roselyne Bachelot.
These evolutions were contested by other medical unions, especially the leading organization CSMF, which played an active role in the withdrawal of the “health contracts” as well as the “referring physician”. The alliance with the Minister Bachelot in 2008 was also contested inside MG France union because of its limited results and led to the resignation of the leader of the union, Martial Olivier-Koehret.
The emergence of new medical organizations representing young physicians since the 1990s also played an important role in this political process. They are less focused on the coordinating role of GPs than on the issues of team practice with other healthcare providers, better working conditions, social protection for physicians (especially maternity leave), and integration between medical practice and medical research. These new organizations have gained access to the ministry of Health
10 and are progressively associated with the discussion of the national medical agreement (but without the power to sign it). These changes in the physician union movement are key to understanding the emergence of an instrument constituency in the structuration of primary care in France.
The Structuration of an Alliance of Governmental and Professional Actors around the MSPs as a Policy Solution
Beyond the political positioning of MG France and young physicians’ unions on the political scene, some MG France members have led local initiatives aiming to develop multi- professional coordination and a more social and preventive approach to healthcare. After a first, and not very conclusive, attempt in the 1980s to organize specific patients’ pathways between the outpatient and hospital sectors within the framework of healthcare networks
11, some GPs—most of them members of MG France—set up informal team practices with other healthcare providers (mainly nurses and physiotherapists, and sometimes midwives, psychologists, dental surgeons and specialist physicians). We interviewed these pioneers and identified their main motivations: to attract young GPs likely to be interested in team practice and to better coordinate and organize patient care pathways according to each one’s preferences and competences with the aim of better distributing the workload. They also see these changes as a way of improving care quality and responding to the growing challenges of aging and chronic diseases, which GPs cannot tackle alone. One of them, leader of one of the first informal team-based organizations, explained:
“The demand for care is becoming more complex and we realize that we cannot work alone. Thirty years ago, it was simple because we were confronted with typical pathologies. Today it is becoming more and more complicated, and so the vision of other professionals, with other experiences, will allow me to consider the issue differently. I’m very limited on my own if I don’t have the advice of a nurse, the intervention of the pharmacist, the social worker, et cetera, et cetera. So, to say it quickly, I think this evolution is a logical evolution (…). With the increasing complexity of healthcare, at some point we are forced to team up. Physicians and other professionals come to it, gradually, by necessity. But this adaptation is very late. The profession is 20 years late. Hospitals and clinics have already made great strides regarding these issues, they already have developed multi-professional responses. For example, staff meetings in cancerology have existed for years. Whereas in primary care, multi-professional meetings only began with the MSPs.”
(Pierre de Haas, GP, male, over 60, leader of an informal team- based organization in Pont d’Ain, former national secretary of MG France union, and second president of the national federation of MSPs, interview conducted in 2017)
Our interviews with other GPs who followed these pioneers and set up their own coordinated practices confirm the central objective of attracting young colleagues in order to reduce the pressure on GPs already in practice and ensure the sustainability of medical provision.
“Why did we do all this? asked one of them. So that the supply of care would be maintained. Because even medical group practices like ours were in danger. When someone was leaving, they were not replaced. But here in the MSP, the way we work attracts young people. Because we can take time off whenever we want because there’s always someone, and we can discuss patients’ cases. It corresponds to the desire of young doctors. We already didn’t want to work like our fathers, but even less so now.”
(GP, male, over 60, who led a MSP project in the 2010s in the Paris suburbs, interview conducted in 2017)
And indeed, the possibility of integrating a multi-professional practice is a key motivation for 73% of physicians under 40 years of age, as opposed to only 27% of those over 60 (
Chaput et al., 2020), demonstrating the interest of younger generations in this type of organizations.
In 2006, two members of MG France (Dr. Serin and Dr. De Haas—mentioned above) created a national federation (first called Fédération Nationale des Maisons de santé before becoming the Fédération française des maisons et poles de santé in 2008, FFMPS, and being renamed AVEC Santé in 2018) with a twofold mission: on the one hand, it supports healthcare providers who wish to set up team- based organizations locally; on the other hand, it promotes this new model vis-à-vis the public authorities. This federation has rapidly established itself as a key partner for institutional actors (
Vezinat, 2019): its representatives (mainly GPs but also other health providers) were soon invited to participate in meetings and working groups with administrative officials at the national and regional levels, and reciprocally, political and administrative actors began to attend the federation’s symposium every year. This reconciliation is not actually based on a shared understanding of the situation and common interests between the Welfare elite and the professional entrepreneurs, but rather on an alignment of their different interests, which drive them to advocate the same policy solution with functional (problem solving) and structural (strengthening both actors) promises (
Voß & Simons, 2014). For the former, MSPs are likely to attract young physicians to address difficulties in accessing care. For the latter, the primary goals are to enhance the role of GPs in the healthcare system and improve their working conditions (
Moyal, 2026). Although the relationship between MG France and the FFMPS is obvious, the federation brings together a wider range of GPs interested in team practice as well as other healthcare professions: nurses, physiotherapists, etc. Representatives of the two main unions standing for GPs (MG France and the GPs’ branch of the CSMF) we interviewed stressed the importance of relying on an independent organization to defend this mode of practice, and distancing themselves from the “confrontational” approach typical of union politics, instead positioning themselves as partners with public authorities in the process of organizing primary care (
Moyal, 2026):
“We needed leaders, both at the local and national levels, who want to make things change. [At the local scale] the leader makes the other professionals aware of the problems and drives the group. But we also needed national leaders. And it was Pierre De Haas, clearly. For me, the federation was a major player. It enabled us to move forward much more quickly, because we were negotiating directly with the Ministry of Health.
(Dr. Luc Duquesnel, GP and president of the GPs’ branch of the CSMF, at the origin of a team-based organization in Mayenne, interview conducted in 2017)
“Through unions, we remain in a confrontational relationship with the government, whereas it is absolutely essential, I think, that we work in partnership. With the federation, those of us who wanted to work with public authorities gradually distanced ourselves from unionism. The federation’s annual conference in 2015 marked the climax of this story, with an official visit from Marisol Touraine (then Minister of Health). The federation was—finally! —recognized by the government as an essential partner. And this coincided with a very interesting phase, with people in the social security administration launching an experiment with new remunerations for coordination. (…) So there was a combination of events and people in different places that made it possible to move away from a permanent confrontation between professional organizations and public authorities.”
(Dr. Pierre De Haas, interview conducted in 2024)
At the same time, the Ministry of Health was showing increasing concern about the difficulties in accessing primary care and more specifically GPs, and the resulting delay in treatment for patients and inappropriate use of emergency rooms in hospitals. This situation has an impact not only on population health but also on the level of health expenditure
12. This problem is not exactly new, as we note some concerns in the press and in the political arena from the 1970s onwards about the unequal distribution of GPs across the country. But it remained a latent problem until the 2000s, when several public reports highlighted growing difficulties of access to medical care in certain areas, mainly rural areas and disadvantaged urban neighborhoods, under the combined effect of different factors: the introduction of a mechanism limiting the number of physicians graduating each year (called
numerus clausus13), an increasing number of physicians retiring, and changes in working arrangements (reduced working hours, diversification of activities, choice of settlement location, etc.) (
Berland, 2005;
Berland & Gausseron, 2002;
HCAAM, 2004;
ONDPS, 2004). While these reports refer to situations of “deficits” or “shortage” in medical provision, they also use the more evocative expression of “medical deserts”, which contributes to the “dramatization” of the problem and its legitimation on the political agenda (
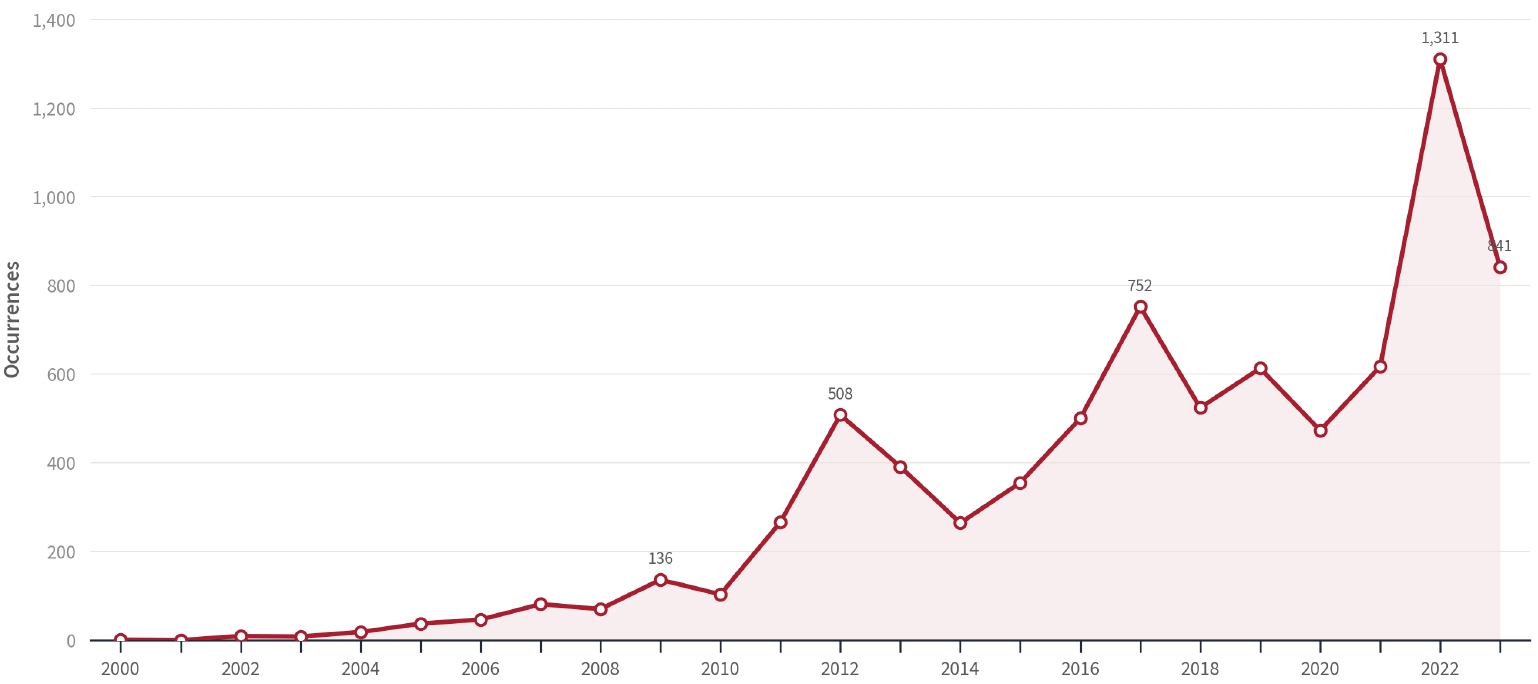
Hassenteufel et al., 2020a). Meanwhile, the medical deserts became widespread in the press. Our analysis over two decades, from 2000 to 2023, shows that this expression is increasingly used in national newspapers, with peaks at each presidential election in 2012, 2017, and 2022 (see
Figure 1). Simultaneously, half of the 10 candidates in the 2012 election and 9 out of 11 candidates in the 2017 election mentioned the medical deserts in their political speeches or programs (
Moyal, 2024). Medical deserts have thus become a major electoral issue at the national level. And this is also true at the local level: a survey conducted by France Assos Santé
14 and the CSA polling institute ahead of the 2026 French local elections shows that healthcare is the most important concern among French people (for 70% of them), before security (for 68%). When asked what their mayor’s top priority should be, 37% of French people first mentioned maintaining and expanding access to healthcare (
France Assos Santé & CSA, 2025).
To address this problem, the French government first promoted solutions aimed at improving the volume of medical provision, by increasing the number of physicians graduating each year, making family medicine more attractive (see the second part of this paper), and providing financial incentives for GPs to settle in certain deprived areas (increased fees, installation bonuses, and tax exemptions). However, the government progressively turned to more organizational solutions (
Moyal, 2026). The public reports we mentioned above, which highlighted the problem of local shortages of GPs, also emphasized the lack of coordination with other professionals. They advocated for the development of team practice and mentioned the local experiments carried out by some GPs. These team-based practices were not only seen as a way to attract young physicians, but also to facilitate the transfer of tasks from GPs to other professionals—more numerous—in order to offset the medical shortage (
Berland, 2003).
A 2007 Senate report (
Juilhard, 2007) draws on a survey conducted the same year by the French Medical Council (CNOM
15) to promote this new kind of team-based organizations. It concludes that 93% of young doctors (medical internes and newly licensed doctors) consider working in this type of structures to be a motivating factor when deciding where to set up practice, ahead of financial incentives (
CNOM & BVA, 2007). “
For several years now, the report states, collective practice has taken a new form: that of the healthcare homes, a concept that has not been defined but that has met with real success among healthcare professionals and local elected officials” (Ibid., p. 39). This report finally gives a voice to some GPs who have informally developed such coordinated practices, and among them Dr. Serin and Dr. de Haas. For them, politicians have leveraged their initiatives because they saw them as a means of achieving their objective of reorganizing outpatient care by avoiding coercion, in particular without interfering with the physicians’ freedom of settlement. Dr. De Haas comments:
“I believe that politicians have seized on the MSPs that were appearing here and there, because they were totally helpless. There is a real delay in terms of services, and politicians know it because they are patients themselves and they hear their fellows. And they are helpless, they cannot find the key because they are faced with liberal professionals, who are free to establish themselves wherever they want to. And politicians wonder how to deal with the problem, but all of a sudden, they see the MSPs and think it’s the solution to all the problems. The only ones who had another solution were a team of deputies who dared to talk about regulating physicians’ settlement! And by the way, I think this would be the only real solution. It would be to say: “It’s a mess, everyone must be salaried and the State takes over”. But could you imagine the protest? Because there is a historical opposition between the State and the medical profession. Politicians have always been afraid of healthcare professionals, because of all the protests. My whole generation remembers the protest on the Alexandre III bridge [in Paris] in the 1980s, when the police charged the doctors. The result is that politicians don’t know how to deal with the organization of primary care and they need professionals to find the solutions. So we’re a few leaders in the profession doing that, particularly through our Federation [see below], and politicians support us.” .
(Dr. Pierre De Haas, interview conducted in 2017)
Meanwhile, political and administrative actors also promoted this new mode of practice. The 2007 LFSS and the 2009 HPST Act—which are notably inspired by the 2007 Juilhard Report’s conclusions— gave a legal recognition and framework to team-based practices, now referred to as “multiprofessional healthcare centers” (
Maisons de Santé Pluriprofessionnelles, MSPs). The Ministry of Health defined guidelines for team practices seeking official recognition and launched a pilot program to compensate private providers working in these organizations for the time they dedicate to coordination and public health activities, which could not previously be valued in a fee-for-service scheme. This program was called “New Remuneration Methods Experiment” (ENMR
16) and supplemented fee-for-service payments, which continued to represent most of the professional income. The ARSs supported the implementation of MSPs and the ENMR at the local level: they established medical zoning to identify priority areas where MSPs should be promoted, allocated subsidies to support healthcare providers who decide to set up MSPs, and selected the structures that would participate in the new remunerations experiment. Local sickness funds took over in 2017 through a national agreement—which was for once interprofessional, representing the various professions working in MSPs—setting out the criteria these structures must meet in order to obtain the new remunerations. This new scheme took the form of a contract healthcare providers can sign with local sickness funds, called ACI
17.
Finally, although the interests of the healthcare administration and GPs may differ—the former seek to improve healthcare access and efficiency, while the latter are most interested in improving their working conditions and positioning themselves as the gatekeepers and coordinators of the system—they eventually converge on a common solution and set up an “instrument constituency” (
Béland & Howlett, 2015;
Voß & Simons, 2014) around MSPs. The recognition of the problem of medical deserts in the political and public agenda allowed these new modalities of practicing liberal medicine—until then undertaken informally and advocated by a minority of GPs—to obtain full political recognition as well as a legal and financial framework. This case clearly illustrates the theory of solutions chasing public problems (
Kingdon, 1984), while also offering an opportunity to analyze the alliance of actors with differing interests around a same policy instrument.
The Progressive Institutionalization and Extension of the Instrument Constituency
Beyond the official recognition of MSPs, the 2007 LFSS (Social Security Financing Law) and the 2009 HPST Act mark a turning point in healthcare policies in France. The HPST Act establishes the basis for a re-foundation of both the governance and the organization of the French healthcare system. On the one hand, it completes the process of “territorialization” of health administration that began in the 1990s, by recognizing the administrative “Regions”
18 as the relevant level for the implementation of healthcare policies, and by extending the government’s planning objectives to outpatient care—a former reform in 1996, known as the “Juppé Plan”, having already made significant efforts to plan hospital care. It thus creates the Regional Health Agencies (ARS), which replace the Regional Hospitalization Agencies (ARH). On the other hand, the HPST Act proposes a reorganization based on a gradation of levels of care provision, according to patients’ needs. It distinguishes between primary or front-line care (called “premier recours”), provided by ambulatory providers (first and foremost GPs) and which aim to meet the basic needs of the population, and specialized or second line care, to which front-line providers refer patients if necessary
19. This law also paves the way for formalizing coordination in the primary care sector. It defines for the first time the coordination and referral missions of the “primary care GP” (“
médecin généraliste de premier recours”) and provides new coordination tools that are unprecedented in the outpatient sector, especially cooperation protocols that allow GPs to delegate procedures to other providers on a voluntary basis, exceeding the legally established competencies of each.
Since then, subsequent legal texts—the 2016, 2019, and 2021 Acts
20, the annual Social Security Financing Laws, as well as national medical and interprofessional agreements with the national health insurance fund—have contributed to the double process of territorialization and integration of healthcare services, through measures aimed at fostering coordination both within organizations and local areas. More specifically, the 2016 Act recognizes new forms of teamwork through the Primary Care Teams (
Équipe de Soins Primaires, ESP), which brings together providers from the ambulatory sector who are willing to coordinate around specific issues (for example the management of a particular pathology or population, or the demand for walk-in medical care) without committing to a contract with the public authorities as required within the MSP framework. The same Act also sets up new local networks aimed at improving care services integration for areas of 40,000 to 200,000 inhabitants: the Local Professional Health Communities (CPTS
21). Healthcare providers and social workers affiliated with these local networks—which sign contracts with the local health insurance funds just like the MSPs —are mandated to guarantee better access to care (more specifically to referring GPs), to improve patient pathways between outpatient care, hospital care, and social services, and to develop prevention.
The 2018 LFSS then introduced new experimental subsidies to encourage GPs in team-based structures to make their practices evolve (in terms of quality of care, patient retention, etc.) and coordinate better with other care providers through the PEPS pilot program (Paiement en équipe de professionnels de santé), and to incentivize coordination between outpatient and hospital sectors through the IPEP pilot program (Incitation à une prise en charge coordonnée). In her recent work on the PEPS and IPEP experiments, Noémie Morize shows that the same instrument constituency united around MSPs is at work here, joining forces this time with economists who are involved in developing these new economic models (
Morize, 2025).
The institutionalization of this instrument constituency can be related to important administrative transformations which strengthen the management of primary care issues. On one side, the scope of operation of the healthcare administration has evolved and now includes the ambulatory sector, in addition to hospital and medico-social services. The Ministry of Health’s “Department of hospitalization and organization of care” (DHOS
22) became the “General department of health care provision” (DGOS
23) in 2010, while the Regional Hospitalization Agencies (ARH) were replaced by the Regional Health Agencies (ARS) in 2009, as mentioned above. On the other side, within the DGOS, the ARS as well as the local health insurance fund (CPAM), specific units dedicated to primary care were created, quickly becoming the first points of contact for private healthcare providers who wish to switch to these modes of practice. They are expanding their role from financing and regulating healthcare to include a support function. This is illustrated by the introduction of “coordinated care referents” in the local health insurance funds (CPAMs) in 2019. Although these changes are reflected in the organizational diagrams of these institutions, they correspond to very different realities from one territory to another, and have not yet made it possible to overcome a traditionally regulatory and top-down culture of their civil servants (
Bontemps, 2020). These changes are, however, a sign of the gradual adaptation of the traditional programmatic actors to the intervention of professional entrepreneurs in the structuration of primary care.
Meanwhile, the scope of competences of non-medical professionals is expanding, particularly nurses
24 and pharmacists: first, through exceptional delegations from physicians to other healthcare providers, covered by the cooperation protocols we mentioned above, allowing to exceed legally recognized professional competencies ; second, with the legal recognition of new competences for non- medical providers. The “advanced practice” scheme for nurses introduced in 2016—inspired by the nurse practitioner model in the US—now allows them to take responsibility in the management of stable chronic conditions, chronic kidney disease, dialysis, and kidney transplantation, in oncology, and, more recently, in psychiatry. Following the same path, a new bill voted by the French parliament in June 2025 expanded nurses’ scope of responsibility by entitling them to formulate diagnoses and prescribe additional tests and specific health treatments and products. All these measures aim to enable a more relevant use of the professional resources available locally, in a context of increasing shortage of medical provision and changing health needs. However, most medical unions were opposed to the advanced practice scheme for nurses at the time and now reject the legal expansion of their competencies.
These policy developments in primary care have led to an extension of the instrument constituency to other healthcare professionals than GPs as well as elected politicians specialized in healthcare issues, in Parliament and in local authorities. On the one side, non-medical providers have gradually gained influence in strategic decision-making of the MSP federation (Avec Santé): the federation’s leadership is now shared among GPs, nurses, and physical therapists. On the other side, while the movement of administrative decentralization of the healthcare system, which began in the 1980s, initially caused reticence among elected representatives who feared becoming solely responsible for the growing demand for healthcare (
Pierru, 2010), they are increasingly involved in the development of primary care and, above all, of MSPs. The 2022 “Differentiation, Decentralization, Deconcentration and Simplification (3DS) Act” strengthened the role of local authorities, through the right to finance healthcare provision and medical staff and strengthened their representation in the ARSs’ boards. This is a response to the claims of elected officials during the national consultation “Ségur de la santé”, which was organized by the Ministry of Health just after the end of the first Covid-19 lockdown in May 2020 (
Hassenteufel, 2024)
25.
The ongoing reform of primary care is thus accompanied by a reconfiguration of the relations between the programmatic “Welfare elite”—i.e. the political and administrative actors at the central level who have carried out the main healthcare reforms since the 1980s—, the political actors at the local level—which are more and more “offensive” in the conduct of public policies (
Le Lidec, 2007)—, and the healthcare providers—who are organizing themselves collectively and are now in a position to form new alliances in order to defend or oppose modes of practices that break away from their traditional ones.
The Recent Weakening of the Instrument Constituency
This repertoire of instruments in primary care, extending MSPs, coincides with the emergence and structuration of new policy actors, while the established ones evolve, ultimately impacting the established alliances among them. New professional organizations are emerging alongside the traditional medical unions and the MSP federation AVEC Santé. In 2010, the former leader of MG France (Dr. Martial Olivier-Koehret) created an association promoting coordinated care (called association “Soins coordonnées”), which has not received the same attention as the FFMPS. And in 2016, another member of MG France (Dr. Philippe Marissal) created the Primary Care Federation (“Fédération des soins primaires”) aiming to promote primary care more widely and to defend diversified coordination models beyond MSPs—but this federation quickly suspended its activities. A few years later, professionals who are organized in CPTS have created their own federation (the Fédération des Communautés Professionnelles Territoriales de Santé, FCPTS), which was initially headed by a member of MG France (Dr. Claude Leicher), then replaced by a nurse (David Guillet) and recently by another GP (Dr. Jean- François Moreul). It receives increasing attention from public authorities. While the organizational model advocated by this Federation does not contradict MSPs, CPTS are likely to relegate MSPs to a secondary position in the primary care reform process (
Fournier et al., 2025;
Moyal & Fournier, 2022). Furthermore, the shaping of these federations shows that the professional entrepreneurs promoting MSPs are no longer the sole leaders of this organizational process. They are progressively joined by other healthcare professionals, who position themselves in favor of team practice and extended competencies for other professions. Unions representing nurses, pharmacists, midwives, chiropodists, orthoptists, and biologists signed the interprofessional agreement in 2017 (ACI) along with physicians’ unions (MG France and the CSMF) and the national sickness fund, allowing the new collective remunerations in MSPs
26. One year later, another agreement was signed by a wider range of professional organizations
27 supporting the development of coordinated care, not only in MSPs but also in CPTS and Primary care Teams (ESP).
More recently, local elected officials and members of parliament have been advocating for regulatory measures on GPs (and other medical specialists) settlement, whereas MSPs were specifically designed to circumvent coercive measures. For a few years now, successive bills introduced by cross-party members of parliament call for an end to the incentive-based approach, which they believe has failed to achieve its objectives. However, the government has so far rejected such coercive measures, echoing the medical profession’s argument that they would act as a deterrent for younger generations, who might turn away from family medicine (
Moyal, 2026). Medical unions from all sides, including MG France that had previously been the most open to these changes, form a united front against these proposals.
These changes in France’s primary care sector finally seem to face several obstacles, which are fueled by the persistence of the medical deserts’ problem on the political agenda. The “MSP solution” has not been able to establish itself as a sufficient answer to the problem of access to healthcare. The salience of this issue has triggered its politicization at the national and local levels and has made it more acceptable to debate the regulation of settlement of physicians in outpatient care. The most recent illustration is a multipartisan legislative initiative “aiming to tackle medical deserts”, including the principle of administrative authorization for settlement, which was voted in the National Assembly in May 2025 and submitted to the Senate. It has provoked equally strong opposition from the organizations defending the historical principles of “free medicine”. They are joined by the leaders of MG France who express loudly that GPs feel blamed by attempts to coerce them, “accused of never doing enough” while feeling overwhelmed by work, and put “in competition” with other professions whose prerogatives are expanding while the role of the primary care physician is becoming ambiguous
28. The resurgence of the cost-containment agenda (with discussion around constraining measures for physicians) in the post-pandemic context—the French healthcare system’s deficit reached 15 billion euros in 2025—is further straining relations between the government and the medical profession. In January 2026, a massive physicians’ strike —which is unprecedented considering the united front formed by professional organizations that are traditionally divided —is likely a sign of a deep rift between the initial actors forming the instrument constituency that has led primary care reforms since the 2000s. GPs, represented by MG France and the CSMF, have aligned themselves behind the demands of traditionally more liberal organizations representing specialist physicians. The medical profession is unanimously calling for a revaluation of medical procedures, complete freedom to set up practice, and relief from certain tasks considered time- consuming (such as issuing sports fitness certificates).
Another fragility of the instrument constituency is that administrative actors rarely specialize in primary care and subsequently switch to other aspects of the healthcare system, particularly healthcare financing and hospital organization (
Morize, 2025).
Conclusion
From a more general theoretical perspective, this paper highlights two main factors explaining the weakening of an instrument constituency, a dynamic which has been less analyzed than institutionalization. The first one is the persistence of the policy problem (in our case “the medical deserts” issue) that has sustained the shaping of an instrument constituency, in a solution chasing problem process. It weakens the functional promise of the policy instrument which seems unable to address adequately the problem and exacerbates conflicts. The second factor is the increasing number of policy actors aiming to tackle the same issue and promoting a wider range of less consensual policy instruments. Paradoxically, the institutionalization of the instrument constituency can also be a factor of its progressive destabilization as our empirical case shows.
Second, it provides a new instrument constituency example with strong professional dimensions: professional entrepreneurs and professional interests are playing a key role in the structural promises of this policy instrument. Usually, the notion is used for cases with a strong expertise dimension and for market-oriented instruments, unlike the MSP, which is more akin to an organizational instrument. It raises the question of the conditions of the structuration of that kind of instrument constituency. Two have been pinpointed in our analysis: the salience of a policy problem—with the “medical deserts” issue—and the role of professional entrepreneurs in the shaping of an organizational model addressing multiple issues—not only the lack of medical workforce but also working conditions, improvement of patient care through coordination and prevention. This helps to explain, in part, the differences compared to Bismarckian healthcare systems, where new primary care organizations have not been supported by an instrument constituency. It is the case in Germany where the model of the MVZ (Medizinische Versorgungs Zentren) is met with greater resistance from professional actors, as it paves the way for the involvement of economic operators in a context where the issue of medical shortage seems less politicized (
Hassenteufel et al., 2020b). In an analytical generalization perspective, the French case suggests three scope conditions for the formation (or non-formation) of instrument constituencies in primary care reform across Bismarckian health insurance systems. The first dimension is the degree of politicization (and dramatization) of medical workforce shortages; the second the presence of professional entrepreneurs willing to partner with state actors rather than acting solely as veto players; and the third the shaping of an instrument that guarantees the preservation of physicians’ professional autonomy.
Finally, the paper sheds light on the importance of interdependency between policy actors for healthcare reform in a Bismarckian health insurance system. The analysis provided in this paper leads us to argue that a primary care reform process in France could not be initiated without the congruent involvement of the political and administrative actors who traditionally oversee the design and implementation of healthcare and social reforms in this national jurisdiction (
Genieys & Hassenteufel, 2015;
Marier, 2005), on the one hand, and the medical profession, on the other hand, which has always had the freedom to establish practices and organize itself, especially in this predominantly private sector. As long as the system guarantees the principles of private medical practice this alliance may remain favorable to the medical profession, whose support is necessary to carry out reforms. Professional entrepreneurs are actually driving the transformation of primary care since the 2000s, supported by the Welfare elite attempting to take advantage of it. However, recent legislative changes (recognizing expanded competencies for other professions and seeking to regulate physicians’ freedom to set up practice) could weaken the medical profession’s power and its primary role in this reform process.
The “complex bargaining process” —which characterizes the interdependent relationship between French GPs and the Welfare elite and underpins the reform process in this sector (
Moyal, 2024, p. 1044) —could therefore be compromised. It sheds light on the limits of the institutionalization of the programmatic Welfare elite in France, based on the creation of new steering, expert, and implementation institutions and the circulation of its members between them makes it possible to understand the continuity over time of different generations of this group (
Darviche et al., 2022). The shifting of the key policy issues in French healthcare policies, accelerated by the Covid-19 crisis, has weakened the autonomy of the programmatic elite (Bandelow & Hornung, 2020), which has to build new alliances with professional actors and depends more on political actors, not only at the local level for the implementation of new policy instruments but also at the national level with the fragmentation of the French political landscape leading to increasing political instability (since 2022 health policy actors have experienced 6 different Ministers in charge of the healthcare sector).
Notes
Figure 1.
Use of “medical deserts” in the French press from 2000 to 2023
Source: (Moyal, 2024). Analysis conducted using the Factiva database.
Note: Newspapers searched: L’Humanité, La Croix, Ouest France, Libération, Le Monde, Les Echos, and Le Figaro.
Search terms: “déserts médicaux”, “désert médical”, “désertification médicale”, and “pénurie médicale”.
References
- Bandelow, N. C., & Hornung, J. (2020). Policy programme cycles through old and new programmatic groups. Journal of Public Policy, 41(4), 633–652. https://doi.org/10.1017/S0143814X20000185
- Becker, H. (1966). Social problems: A modern approach. Wiley.
- Bergeat, M., & Cassou, M. (2023). Un tiers des médecins généralistes, et plus de la moitié de ceux exerçant en MSP, collaborent quotidiennement avec des infirmières [Technical report].
- Berland, Y. (2003). Rapport de la mission « Coopération des professions de santé »: Le transfert de tâches et de compétences (rapport d'étape) [Technical report].
- Berland, Y. (2005). Rapport de la commission « Démographie médicale [Technical report].
- Berland, Y., & Gausseron, T. (2002). Rapport de la mission « Démographie des professions de santé [Technical report].
- Bloy, G. (2010). La constitution paradoxale d'un groupe professionnel. In Singuliers généralistes: Sociologie de la médecine générale: Singuliers généralistes: Sociologie de la médecine générale (pp. 21–40). Presses de l'EHESP. https://doi.org/10.3917/ehesp.bloy.2010.01.0021
- Bontemps, A. (2020). Accompagner la structuration des soins primaires après la Covid-19: Un nécessaire renversement du fonctionnement des institutions publiques de la sant. Regards, 1(57), 225–241. https://doi.org/10.3917/regar.057.0225
- Borgetto, M. (2011). La médecine libérale, quel avenir?. Revue De Droit Sanitaire Et Social, Hors série.
- Béland, D., & Howlett, M. (2015). How solutions chase problems: Instrument constituencies in the policy process. Governance, 29(3), 393–409. https://doi.org/10.1111/gove.12179
- Chaput, H., Monziols, M., Ventelou, B., Zaytseva, A., Chevillard, G., Mousquès, J., Fressard, L.; others (2020). Difficultés et adaptation des médecins généralistes face à l'offre de soins [Technical report].
- CNOM, & BVA (2007). Attentes, projets et motivations des médecins face à leur exercice professionnel [Technical report].
- Darviche, M.-S., Genieys, W., & Hassenteufel, P. (2022). L'institutionnalisation de l'élite du Welfare au coeur de l'État. Les nouveaux gardiens des politiques d'assurance maladie. Revue Française De Science Politique, 72(5), 701–721. https://doi.org/10.3917/rfsp.725.0701
- Fournier, C., Bourgeois, I., & Naiditch, M. (2018). Action de santé libérale en équipe (Asalée): Un espace de transformation des pratiques en soins primaires. Questions D'économie De La Santé, 232, 1–8.
- Fournier, C., Morize, N., & Moyal, A. (2025). France: Multiprofessional primary care groups and the long path to team practice. In V. Amelung, V. Stein, E. Suter, N. Goodwin, R. Balicer, & A.-S. Beese (Eds.), Handbook of Integrated Care: Handbook of Integrated Care (pp. 1635–1655). Springer Nature. https://doi.org/10.1007/978-3-031-96286-8_111
- France Assos Santé, & CSA (2025). La connaissance et les attentes des Français sur les compétences des maires en matière de santé. https://www.france-assos-sante.org/wp-content/uploads/2025/11/CSA-pour-France-Assos-Sante-Attentes-municipales-et-sante-0611-Lecture-seule.pdf
- Freidson, E. (1970). Profession of Medicine. A Study of the Sociology of Applied Knowledge. Dodd, Mead & Co.
- Genieys, W., & Hassenteufel, P. (2015). The shaping of new state elites: Healthcare policymaking in France since 1981. Comparative Politics, 47(3), 280–295. https://doi.org/10.5129/001041515814709301
- Gusfield, J. (1981). Drinking driving and the symbolic order: The culture of public problems. University of Chicago Press.
- Hall, P. (1993). Policy paradigm, social learning and the state. Comparative Politics, 25(3), 275–296. https://doi.org/10.2307/422246
- Hassenteufel, P. (1996). The medical profession and health insurance policies: A Franco-German comparison. Journal of European Public Policy, 3(3), 461–480. https://doi.org/10.1080/13501769608407044
- Hassenteufel, P. (1997). Les médecins face à l'État: Une comparaison européenne. Presses de Sciences Po.
- Hassenteufel, P. (2010). La difficile affirmation d'un syndicalisme spécifique aux généralistes. In Singuliers généralistes: Sociologie de la médecine générale: Singuliers généralistes: Sociologie de la médecine générale (pp. 403–418). Presses de l'EHESP. https://doi.org/10.3917/ehesp.bloy.2010.01.0403
- Hassenteufel, P. (2019). Les syndicats de médecins entre défense et dépassement de la médecine libérale. Les Tribunes De La Santé, 1, 21–33. https://doi.org/10.3917/seve1.059.0021
- Hassenteufel, P. (2024). Sociologie politique de l'action publique (3rd ed.). Armand Colin.
- Hassenteufel, P., Schweyer, F.-X., Gerlinger, T., & Reiter, R. (2020a). Les « déserts médicaux » comme leviers de la réorganisation des soins primaires, une comparaison entre la France et l'Allemagne. Revue Française Des Affaires Sociales, 1, 33–56. https://doi.org/10.3917/rfas.201.0033
- Hassenteufel, P., Schweyer, F.-X., Gerlinger, T., Henkel, R., Lückenbach, C., & Reiter, R. (2020b). The role of professional groups in policy change: Physician's organizations and the issue of local medical provision shortages in France and Germany. European Policy Analysis, 6, 38–57. https://doi.org/10.1002/epa2.1073
- HCAAM (2004). Rapport du Haut Conseil pour l'Avenir de l'Assurance Maladie pour 2004 [Technical report].
- Jobert, B. (1992). Représentations sociales, controverses et débats dans la conduite des politiques publiques. Revue Française De Science Politique, 42(2), 219–234.
- Juilhard, J.-M. (2007). Offre de soins: Comment réduire la fracture territoriale? — Synthèse du rapport [Technical report].
- Juilhard, J.-M., Crochemore, B., Touba, A., & Vallancien, G. (2010). Le bilan des maisons et des pôles de santé et les propositions pour leur déploiement [Technical report].
- Kingdon, J. (1984). Agendas, alternatives, and public policies. Little, Brown.
- Le Lidec, P. (2007). Le jeu du compromis: L'État et les collectivités territoriales dans la décentralisation en France. Revue Française D'administration Publique, 1, 111–130. https://doi.org/10.3917/rfap.121.0111
- Marier, P. (2005). Where did the bureaucrats go? Role and influence of public bureaucracy in Swedish and French pension reform debate. Governance, 18, 521–544. https://doi.org/10.1111/j.1468-0491.2005.00290.x
- Moran, M. (1999). Governing the Health Care State: a Comparative Study of the United Kingdom, the United States, and Germany. Manchester University Press.
- Morize, N. (2024). Les coûts de l'autonomie: Économistes et médecins libéraux dans les réformes expérimentales des soins primaires. [Doctoral dissertation].
- Morize, N. (2025). Continuities in policies and turnover among actors: Instrument constituencies in French primary care reforms. European Policy Analysis. https://doi.org/10.1002/epa2.70010
- Moyal, A. (2019). Rationalisation des pratiques professionnelles en Maisons de Santé Pluriprofessionnelles: Le paradoxe d'un exercice libéral sous contraintes. Revue Française De Science Politique, 69(5-6), 821–843. https://doi.org/10.3917/rfsp.695.0821
- Moyal, A. (2022). La coopération au coeur du travail entrepreneurial: Le cas des médecins généralistes porteurs de maisons de santé pluriprofessionnelles en France. Revue Française De Sociologie, 63(3-4), 471–499. https://doi.org/10.3917/rfs.633.0471
- Moyal, A. (2024). Implementing primary care reform in France: Bargaining and policy adaptation. The case of MSPs. Journal of Health Politics, Policy and Law, 49, 1015–1050. https://doi.org/10.1215/03616878-11373736
- Moyal, A. (2026). Réguler sans contraindre: L'État et les médecins face aux déserts médicaux. Presses de Sciences Po.
- Moyal, A., & Fournier, C. (2022). Après Ma Santé 2022, encore de multiples défis à relever pour les soins primaires en France. Les Tribunes De La Santé, 71(1), 33–45. https://doi.org/10.3917/seve1.071.0033
- ONDPS (2004). Les effectifs et l'activité des professionnels de santé: Le rapport 2004 [Technical report].
- Pierru, F. (2010). Napoléon au pays du New Public Management. Savoir/agir, 1(11), 29–37.
- Pitti, L. (2021). Le renouveau d'une utopie? Lutter contre les inégalités sociales de santé en médecine générale: Les métamorphoses de la médecine sociale dans les quartiers populaires en France, des années 1970 à aujourd'hui. Revue Française Des Affaires Sociales, 3, 305–317. https://doi.org/10.3917/rfas.213.0305
- Sabatier, P., & Jenkins-Smith, H. (1993). Policy change and learning: An advocacy coalition approach. Westview Press.
- Simons, A., & Voß, J.-P. (2017). Policy instrument constituencies. In Handbook of policy formulation: Handbook of policy formulation (pp. 355–372). Edward Elgar.
- Starfield, B., & Shi, L. (2002). Policy Relevant Determinants of Health: an International Perspective. Health Policy, 60(3), 201–218. https://doi.org/10.1016/S0168-8510(01)00208-1
- Streeck, W., & Thelen, K. (2005). Beyond continuity: Institutional change in advanced political economies. Oxford University Press.
- Vezinat, N. (2019). Vers une médecine collaborative: Politique des maisons de santé pluri-professionnelles en France. Presses Universitaires de France.
- Voß, J.-P., & Simons, A. (2014). Instrument Constituencies and the Supply Side of Policy Innovation: The Social Life of Emission Trading. Environmental Politics, 23(5), 735–754. https://doi.org/10.1080/09644016.2014.923625
Appendix
Table A1. Categories of people interviewed in the two studies
Table
|
REGMEDPROV project (2015–2018) |
MSP project (2016–2019) |
|
Administrative officials |
8 |
6 |
|
Political actors at the national level |
1 |
|
|
Political actors at the local level |
|
3 |
|
MSP federation representatives |
1 |
3 |
|
Other healthcare union representatives |
8 |
9 |
|
Experts (researchers and consultants) |
2 |
8 |
|
Local level practitioners (GPs) |
|
10 |
|
Total
|
20 |
39 |




